- +52 664 761 5349
- contact@tijuanasurgery.com
- Paseo de los Héroes 9211 Edificio Xtal Zona Rio Tijuana BC México 22010
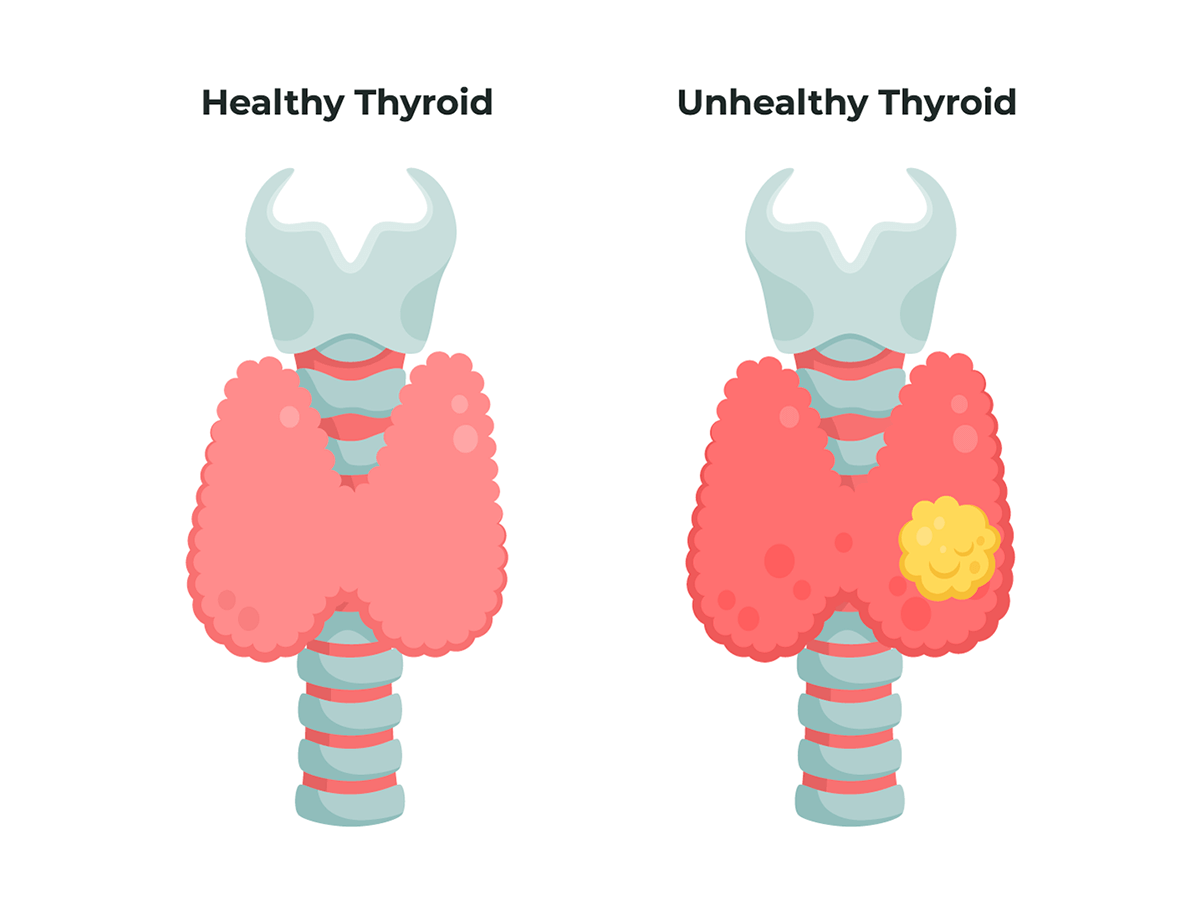
The thyroid gland is shaped like a butterfly and is normally located in the front of the neck. Its job is to form thyroid hormones, release them into the bloodstream and deliver them to all the tissues of the body.
Thyroid nodules are solid or fluid-filled lumps that form inside the thyroid, a small gland located at the base of the neck, just above the breastbone.
Most thyroid nodules cause no signs or symptoms. Occasionally, however, some nodules may become so large that the following is possible:
In some cases, thyroid nodules produce extra thyroxine, a hormone secreted by the thyroid gland. The extra thyroxine can cause symptoms of an overproduction of thyroid hormones (hyperthyroidism), such as these:

Thyroid surgical procedures are indicated for patients with a variety of thyroid conditions, including:
Cancerous thyroid nodules
Benign (non-cancerous)
Large thyroid glands (goiters) and overactive glands
1) Biopsy or removal of a lump – removing a small part of the thyroid gland.
2) Lobectomy – removing half of the thyroid gland.
3) Removing almost all of the thyroid gland (subtotal thyroidectomy-when a small amount of thyroid tissue is left on both sides or near-total thyroidectomy-when about a gram or centimeter of thyroid tissue is left on one side).
4) Total thyroidectomy, in which all identifiable thyroid tissue is removed. There are specific indications for each of these operations.
Thyroid and neck tumor surgery is currently a safe, comfortable and recommended method for most patients, performed through a small incision inside the neck area and with very good functional and aesthetic results.
During thyroid surgery and neck tumors can be performed depending on the case with local anesthesia or in other cases general anesthesia is administered to the patient, the procedure most of the time can be performed on an outpatient basis and the patient can leave the same day and return to work and normal life within a few days.
Dr. Javier Cisneros Lopez is a general surgeon specializing in inguinal hernia in the city of Tijuana, Baja California Mexico with 26 years of experience and more than 7,000 procedures performed. If you have any symptoms or doubts about your health, schedule an appointment here to receive medical attention appropriate to your condition.
It is the H-shaped gland located in the front of the neck. Its function is to produce the thyroid hormone that has an effect on almost all organs, maintaining metabolism. Anatomically it is in close relationship with important structures of the neck such as the trachea, esophagus, carotid artery, internal jugular veins, recurrent laryngeal nerves and parathyroid glands.
The parathyroid glands are very small, usually 4, located behind the thyroid gland. They secrete Parathyroid Hormone (PTH) which is responsible for raising calcium levels in the blood.
Cervical Ultrasound: Ultrasound examination that is able to determine the characteristics of Thyroid Nodules, neck nodules.
Preoperative Ultrasound: It is used in the staging of thyroid cancer. This test shows in detail all the nodules in the neck and their suspected metastasis to be removed in surgery.
Fine Needle Puncture: Procedure performed under ultrasound. A needle is used to puncture the suspicious nodule, taking a sample of cells (cytology), which is analyzed by the pathologist, determining the possibility of a nodule being benign or malignant.
Thyroidectomy is the removal of the thyroid gland, which can be total or partial in selected cases. In this case only one lobe of the gland is removed.
Depending on the size of the cancer, and if there is metastatic involvement in the neck nodules, these must be completely removed along with the gland. This part of the surgery is called cervical emptying or dissection. It may be one-sided or bilateral.
The surgery may also require the use of a rapid biopsy that provides information about the tumor, in case something needs to be changed in the surgical plan.
The surgery is performed under general anesthesia, for this reason, apart from the tests that evaluate thyroid disease, a preoperative evaluation is required with:
Blood tests: hemogram, coagulation profile, glycemia (blood glucose) and creatinine (evaluates renal function).
Electrocardiogram.
Evaluation by specialists to check for any chronic disease, which must be compensated.
Hospitalization, in general, is 1 day. It may be longer depending on how extensive the surgery is.
During the postoperative period it will be necessary to measure calcium levels in the blood on a serial basis and you will have to receive calcium and Vitamin D orally until the function of the parathyroid glands is stabilized.
The use of thyroid hormone may or may not be started postoperatively. It will depend on the final report of the complete biopsy of the tumor. With this it is possible to indicate the use of complementary therapy such as the use of radioactive iodine.
Yes, but it is very rare, and depends on how advanced the thyroid or neck pathology is. Currently there is state of the art medical equipment that is used during surgery to avoid complications of the nerves surrounding the thyroid.
Recurrent Laryngeal Nerve:
Gives mobility to the vocal cords. It has an important anatomical proximity to the thyroid gland, so it must be identified and preserved during surgery to avoid permanent dysphonia. However, it is common for the patient to be left with mild dysphonia postoperatively and to recover with time. Only 1% may be left with permanent dysphonia.
During surgery, a nerve monitor can be used to identify and view the functionality of the nerve intraoperatively. It is an aid, but the surgeon’s experience is more important to avoid its damage.
Hypocalcemia:
All 4 parathyroid glands must be identified and preserved. Postoperative decrease in calcium levels is frequent, even if the glands are preserved. Most of the time it is asymptomatic and recovers with the passage of weeks.
Contact information
Copyrights ©2022 – Tijuana Surgery Center